MEDICAL CASE
This is an E log book to discuss our patient's de-identified health data shared after taking his guardian's signed informed consent. Here we discuss our individual patient problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This e-log book also reflects my patient centered online learning portfolio and your valuable comments in comment box are most welcomed
I have been given this case to solve in an attempt to understand the topic of "Patient clinical data analysis" to develop my competency i reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
CASE DISCUSSION:
A 60year old male came with complaints of
Involuntary movement of B/L upper limbs and lower limbs while driving at late night.
HOPI:
Patient was apparently asymptomatic few hours back and then suddenly developed involuntary movements of B/L upper limbs and lower limbs which lasted for 1hr and came to hospital in an unconscious state and gained consciousness after 2 hrs, but was in a state of confusion until morning 6am.
PAST HISTORY:
K/C/O DM since 10yrs
K/C/O HTN since 8yrs
PERSONAL HISTORY:
He is Married and Bus driver by occupation.
He consumes
- Mixed diet
- sleep is adequate
- Appetite normal
- bowel and bladder movements are regular
- He used to Consume Alcohol occasionally.
FAMILY HISTORY: no similar complaints in the family.
GENERAL EXAMINATION:
Patient is conscious , coherent and cooperative and well oriented to time place
and person,
Moderately built and moderately nourished.
VITALS:
BP: 140/90mmhg
PR: 108
RR: 26
Temp: 99.5f
GRBS: 225mg/dl - 8am
Spo2: 97%
SYSTEMIC EXAMINATION:
RS: BAE+ clear
CVS: s1,s2 no added sounds
P/A: not tender
CNS: pt conscious, coherent
HMF-intact
Reflexes- R L
B ++ ++
T ++ ++
S ++ ++
K ++ ++
A ++ ++
PROVISIONAL DIAGNOSIS: Seizures under evaluation
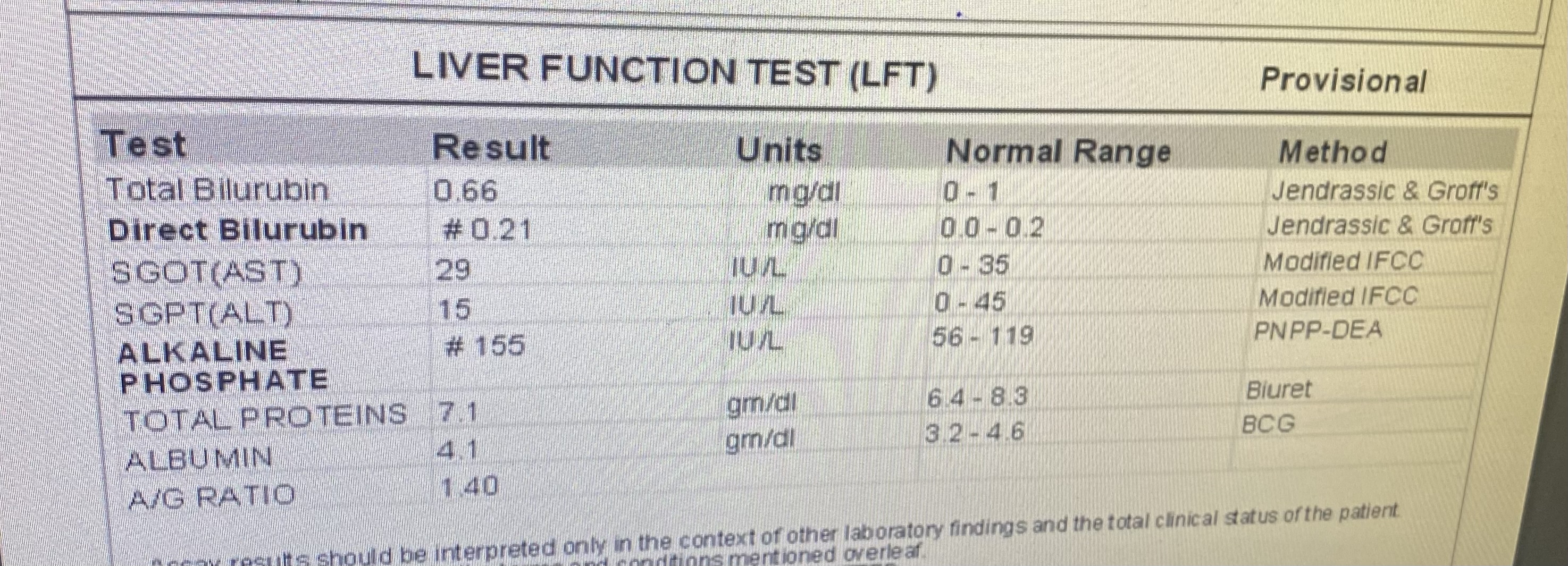
INVESTIGATIONS:
TREATMENT:
1. IV fluids 2 NS 2 RL @75ml/hr
2. Inj.levipil 1gm/iv/stat f/b inj.levipil 500mg/iv/bd
3. Inj. Pan 40mg/iv/OD/BBF
4. Tab.Dolo 650mg/PO/SOS
5. Inj.Human actrapid insulin SC/TID
6. GRBS charting 6th hrly
7. Tab. Prolomet-XL 50 mg/PO/OD
8. Inj. Lorazepam 2mg/iv/SOS
MRI
Course in the hospital: Patient presented with 1 episode of involuntary movements of b/l upper limbs and lower limbs and postictal confusion state. After coming to our hospital patient was given levipill 1gm in 100ml NS infusion for prevention of recurrence of involuntary movements. Further all the test were carried out to know the cause. Organic causes were ruled out as all the tests were in normal ranges. For further evaluation we planned for MRI BRAIN and MRI BRAIN VENOGRAM based on the radiological findings we came to conclusion with lesion in brain in the left side.
Discharge: patient LEFT AGAINST MEDICAL ADVICE as they wanted to get treated in other hospital.
Patient and attenders both were explained about the condition and need for further treatment but they left against medical advice.











Comments
Post a Comment